Retake
R4) New LLQ abdominal pain in a 28-year-old female
Review the Learning Outcomes, Hx, PE and Labs, and begin the module with your Provisional Diagnosis. Keep hitting "Next" to move through the module.
Learning Outcomes
- Articulate your relationship with the consulting diagnostic radiologists in the evaluation of a patient with adnexal pain.
- Review the DDx considerations in a patient with adnexal pain.
- Identify the spectrum of imaging findings in appropriate modalities for evaluating a patient with adnexal pain.
History
The patient is a 28-year-old woman with no significant past medical history presenting for new onset abdominal pain. She reports severe left lower abdominal pain that started 4 hours ago with associated nausea and vomiting. The patient’s last menstrual period was approximately two weeks ago. She is sexually active with her long-term boyfriend, with whom she does not use birth control. She denies any history of sexually transmitted infections. She was previously found to have left hemorrhagic cyst and was recommended to undergo a follow-up outpatient ultrasound.
Physical Exam
BP: 136/82 HR 110, RR 15/min, Temp 98F, O2 saturation 98%.
Left-adnexal tenderness to palpation. There is voluntary guarding but no rebound tenderness or rigidity.
Labs
Urinary β-hCG negative
Provisional Diagnosis
Select the Dx you believe is most appropriate
Ovarian torsion is the most likely diagnosis in this young patient with acute onset abdominal pain, adnexal tenderness, and a negative pregnancy test. This patient’s known adnexal cyst also places her at increased risk for an ovarian torsion.
Well done. You were correct
Potential Acuity
What is your assessment of the likely acuity for this patient?
Well done. You were correct
This patient requires urgent workup and management.
First Imaging Study
What is the first imaging study you will order?
Transvaginal ultrasound is the initial imaging modality of choice because it can effectively assess both the size and structure of the ovaries and adnexal structures, in addition to evaluating blood flow.
Well done. You were correct
Pertinent Imaging Observations
Click on the links below to view images from the study, and assess these key findings as best you can.
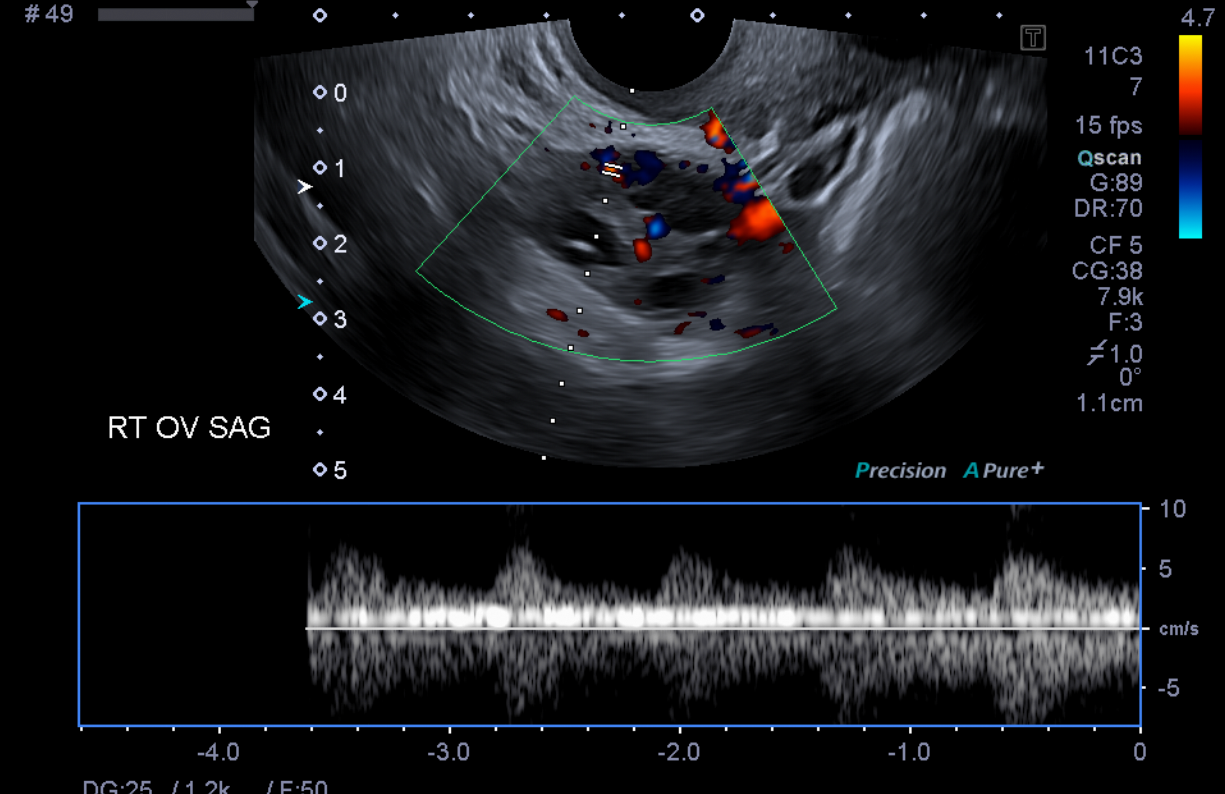
Transvaginal Pelvic Ultrasound with Doppler
There is normal doppler flow in the right ovary.
The right ovary is within normal limits in size and demonstrates appropriate flow.
There is normal doppler flow in the left ovary.
The left ovary demonstrates asymmetrically decreased blood flow.
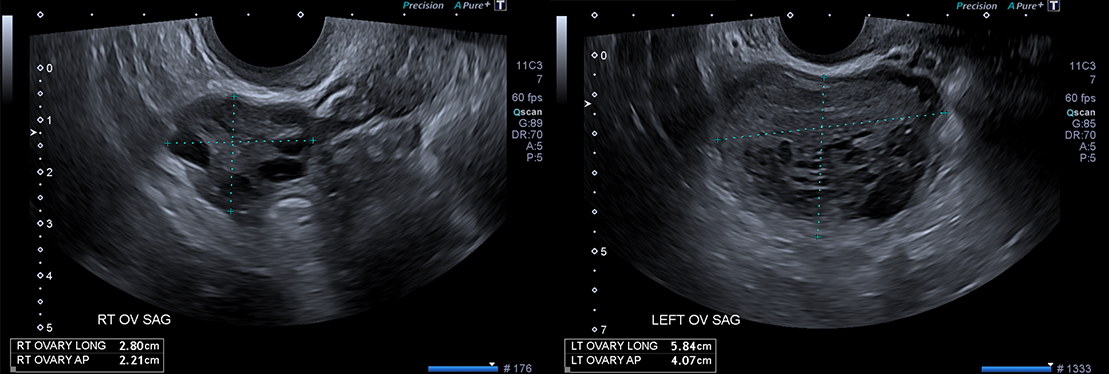
The ovaries are symmetric.
The left ovary is asymmetrically enlarged.
View the full study if you'd like to take a look yourself.
Second Imaging Study
What is the next imaging study you will order?
The ultrasound was suggestive of ovarian torsion, consequently, no further imaging is required. However, if the study were inconclusive, an MRI of the pelvis or abdomen may be considered.
Well done. You were correct
What is your Diagnosis now that you have seen the imaging results?
The imaging findings are most consistent with ovarian torsion. Compromised blood flow to the ovary can result in ischemia and irreversible damage.
Current Acuity
Initially, you selected and we suggested acuity.
Has your concern for this patient changed?
The patient requires urgent workup and management.
Assessment and Plan
Please provide your assessment and plan for this patient
The patient, a 28-year-old woman, presents with acute, severe left-sided adnexal pain and imaging findings indicative of ovarian torsion. An urgent consultation with OBGYN is necessary for potential laparoscopic detorsion, and possibly oophorectomy, if the ovarian tissue is nonviable. Meanwhile, the patient should be managed with analgesics for pain relief, initiated on IV fluids for hydration, and placed on NPO (nothing by mouth) status in anticipation of potential surgery.
Lessons Learned:
- Acute abdominal pain in a reproductive age woman requires urgent work-up to rule out conditions such as ovarian torsion, ectopic pregnancy, PID, ruptured hemorrhagic cyst, and appendicitis.
- The most appropriate imaging technique when ovarian torsion is suspected is a transvaginal or transabdominal pelvic ultrasound with doppler.
- Ovarian torsion can manifest as an asymmetrically enlarged ovary with diminished or absent blood flow.
- If the ultrasound is non-diagnostic and ovarian torsion is still suspected, an MRI of the pelvis without contrast should be performed.
- Normal vascularity may be observed in ovarian torsion due to the dual blood supply from the ovarian artery and uterine artery's ovarian branches.
- Free pelvic fluid is seen in most cases of ovarian torsion.
Socioeconomic Factors: Within the pediatric population, one study showed that patients with public health insurance or no health insurance demonstrated decreased rates of ovarian preservation, or increased rates of oophorectomy.
That's the end of the module! Once you've reviewed the video(s), you can click here for another case challenge.
Next


{kind=link}
{kind=link}
{kind=link}